


This story also ran on InvestigateTV. It can be republished for free.
In early July, as the covid-19 pandemic slammed rural America, the president of a small Kansas hospital sat down on a Friday afternoon and wrote the president of the United States to plead for help.
“I do not intend to add to your burden,” said Brian Williams, a retired Army lieutenant colonel and Desert Storm combat veteran. He said his hospital, Labette Health, was “like a war zone,” inundated with unvaccinated patients. A department head had threatened to resign, saying he could not “watch one more body be carried out.”
But Williams wasn’t seeking pandemic relief.
Instead, he asked President Joe Biden to confront pharmaceutical manufacturers Eli Lilly and Co., Novo Nordisk and others for refusing to honor a federal drug discount program for hospitals and clinics. The program gives Williams millions to pay staff members, ensure remote clinics remain open and provide charity care for patients unable to pay, he said.

“During a global pandemic, I think health care workers deserve a little bit more respect than to have resources taken away,” Williams said in an interview with KHN and InvestigateTV. “Every one of those [drug] companies, I looked them up, and they were not suffering tremendous [financial] losses, as hospitals were.”
Eli Lilly’s stock price increased nearly 40% and the company’s value rose by $59 billion in the first seven months of 2021. In the same period, Labette Health lost $1.2 million in revenue just from the missed savings on prescriptions, Williams said.

Lilly and other manufacturers, though, are holding their ground. They refuse to offer discounts to thousands of hospital-contracted pharmacies, saying the program has grown beyond its intended use and lacks federal checks and balances against duplicate discounts and other abuses. In lawsuits, they contend the billions in discounted sales they provide are rarely passed on to patients and instead are swallowed up by middlemen like contract pharmacies and third-party administrators.
Congress created the so-called 340B program in 1992 to provide extra funding for hospitals and clinics, especially those serving the poor and elderly. The purpose, lawmakers wrote, is to “stretch scarce Federal resources as far as possible, reaching more eligible patients and providing more comprehensive services.”
Companies that want their drugs covered by Medicaid or Medicare Part B are required to offer 340B discounts, typically 25% to 50% off what they might otherwise pay. Hospitals and clinics buy the drugs at the discount and then are reimbursed by an insurance company, Medicare or Medicaid at the higher negotiated rate. The difference is kept by the hospital or clinic to use as it sees fit.
The law does not require patients to benefit directly, a nuance that has fueled great conflict about how the program works and should be regulated.

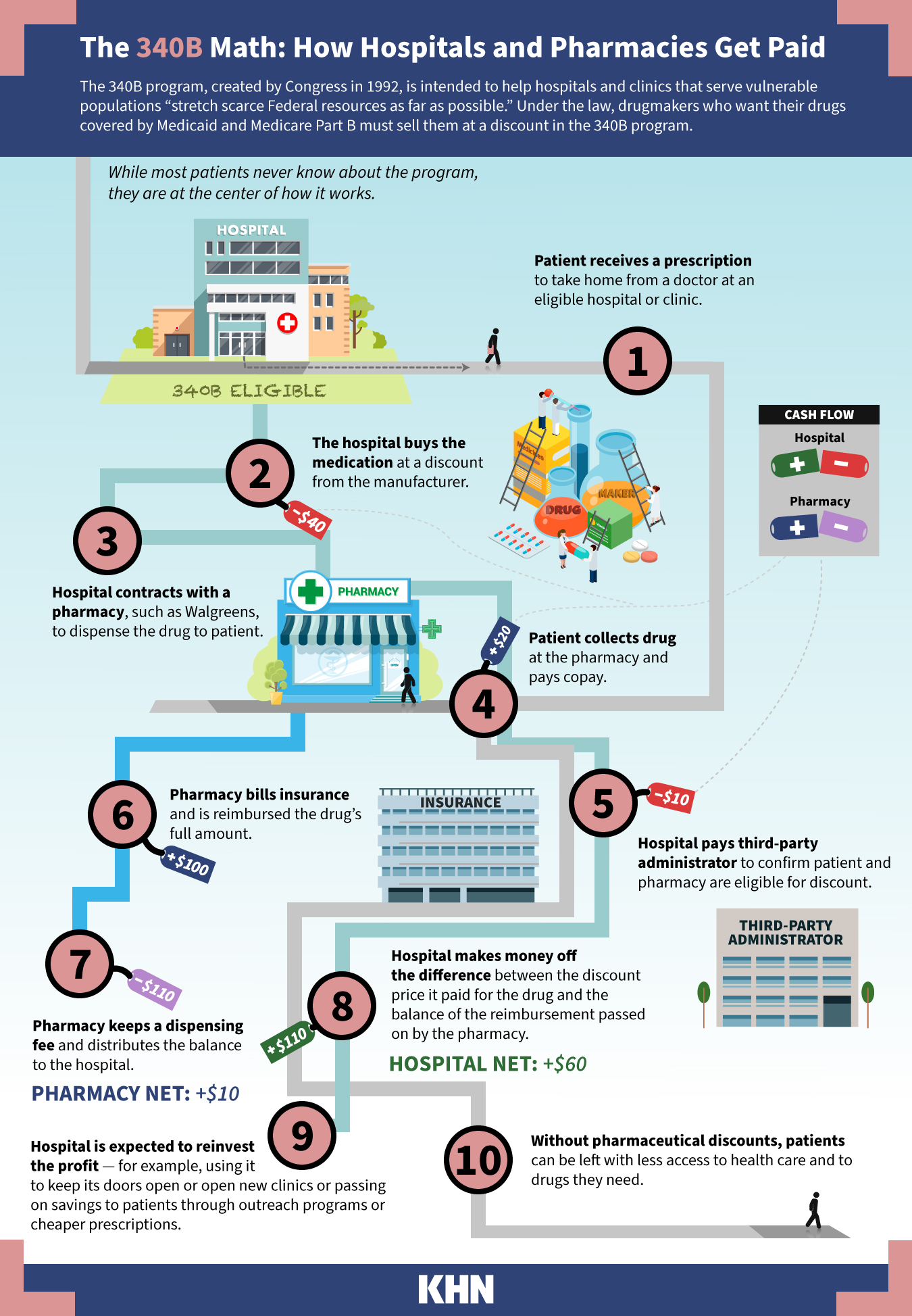
The 340B program’s reach exploded after federal regulators ruled in 2010 that hospitals and clinics could contract with an unlimited number of retail pharmacies such as Walgreens and CVS, which are paid a fee to dispense the discounted drugs. The growth, coupled with long-held questions about regulatory authority, puts the program at a tipping point, with patients stuck in the middle, industry experts say.
The number of pharmacies contracted to work with 340B hospitals to dispense the discounted drugs has soared. It’s reached more than 31,000 nationwide this year from just over 1,700 in 2010, according to an analysis of federal data by InvestigateTV and KHN.
One eye-popping statistic: The drugs purchased under 340B climbed to $38 billion in 2020 from $5.3 billion in 2010, according to the Health Resources and Services Administration, or HRSA, which oversees the program.
Interests on both sides of the program — hospitals and drugmakers — say they are at the mercy of a program designed with the best of intentions, now run amok, hijacked by for-profit companies and wealthy hospitals trying to profit from its largesse.
Adam J. Fein, chief executive of the industry research organization Drug Channels Institute, estimates that nearly half the nation’s retail, mail and specialty pharmacies now profit from 340B: The program, he said, is “essentially taking over the pharmacy industry.”
Legal fights about the program have landed before the U.S. Supreme Court, which is slated to hear arguments this month in American Hospital Association v. Becerra. The hospital industry is challenging a 2018 rule by the Trump administration to cut reimbursement on certain 340B drugs by 28.5%. As Biden’s HHS secretary, Xavier Becerra has upheld the rule.
Most important, the administration says, is to make sure providers use the savings to benefit patients. In an interview with KHN and InvestigateTV, Rear Adm. Krista Pedley, director of the Office of Special Health Initiatives, which oversees the program within Becerra’s agency, said, “We need legislative changes to help make that happen and require that.”
‘Deeply Troubling’
When Sen. Joe Manchin (D-W.Va.) asked during a June appropriations hearing about pharmaceutical companies denying the discounts, Becerra said the drugmakers are violating the law.
“I hope what you’ll do is give us more authority” to regulate the program, Becerra said.
Manchin responded: “I really think we could do that in a bipartisan way, because I’ll tell ya, we’re all being affected.”
As California’s attorney general, Becerra led a coalition of national lawmakers calling for the federal government to hold the manufacturers accountable for their “deeply troubling” actions to undermine the program. At HHS, Becerra put the companies on notice.
Drugmakers — Lilly, AstraZeneca, Novo Nordisk, Sanofi, Novartis and United Therapeutics — took the matter to court, filing several lawsuits. This month, a federal judge ruled that the companies are not required to provide the discounts. A judge in Lilly’s case criticized the “unilateral” action by drugmakers but ruled that the U.S. government’s effort to force them to honor the discounts was invalid.
Notably, U.S. District Court Judge Sarah Evans Barker in Indianapolis wrote that manufacturers believe they are “at the mercy of a system run amok” and that the program “can no longer be held together and implemented fairly” solely through the agency’s guidance and inconsistent messaging.
Becerra requested $17 million annually for 340B program oversight, a $7 million bump. The money would establish a dispute review panel and increase the audits the agency does on manufacturers as well as the providers.
Williams — at his small hospital in rural Parsons, Kansas — said the nearly $4.3 million the hospital gains each year from 340B has allowed him to add a full-time position for case management, increase staffing hours, develop after-school programs and open clinics in impoverished towns that lacked health care.
The hospital has about 20 pharmacies under active contracts, according to the federal database. Williams said it includes locally owned shops like Bowen Pharmacy as well as corporate giants like Walgreens and Walmart, sites that are convenient for patients. A pharmacy added in 2019 is in Frisco, Texas — a mail-order facility that ships specialty drugs directly to patients’ homes.

Patients, Williams said, directly benefit from the federal program: “I’d love to have the CEO of Eli Lilly come here and I’ll take him around and I’ll show him a town of 1,200 where 40% of the population live below the poverty level.”
“Some of our patients come there on a bicycle or in a wheelchair,” Williams said. “I can go 30 minutes in any direction and find pretty tough people living in pretty … pretty austere circumstances.”
One Hospital, 300 Pharmacies
Vanderbilt University Medical Center, based in Nashville, has added three regional hospitals, clinics and providers in recent years — growth that has fueled its rise in contract pharmacies from zero in 2010 to 300 this year. The pharmacies, which reach across Tennessee and all the way to California, “in each instance serve VUMC patients,” Vanderbilt spokesperson John Howser said.

Financial filings do not disclose how much Vanderbilt gains annually from the 340B program, and Howser declined to disclose the amount. The medical system’s operating revenue grew $649 million, or 13%, to $5.5 billion in fiscal year 2021 compared with 2020, according to its latest financial disclosure. Its operating profit rose 25% to $177 million in 2021 compared with 2020.
According to an amicus brief filed in March for the American Hospital Association v. Becerra case, Vanderbilt spends more than $500 million annually on community benefits, such as charity care. Revenue from the 340B program supports low-income programs including medication assistance, home infusion medications and a pharmacy program at a health clinic run by students.
In the brief, Vanderbilt states the government’s cut in Medicare reimbursement has cost the system $12.4 million in 340B savings and will “impact VUMC’s ability to continue to fund community benefit programs at historic levels.”
Large regional health systems have been particularly active in expanding their contract pharmacy networks. The top three — University of Michigan Hospitals and Health Centers, Cambridge Public Health Commission in Massachusetts and Henry Ford Hospital in Detroit — had zero contracts with outside pharmacies in 2010, and each now has more than 500.
InvestigateTV and KHN contacted the 10 providers with the most contract pharmacies and asked why they saw such growth, how much revenue 340B generates and how the money was used.
While some said the money went for charity care and community programs, others did not respond.
Why not require hospitals to report precisely how they use the savings to benefit patients?
It would be “burdensome,” said Maureen Testoni, chief executive of 340B Health, which represents health systems.
She said her organization does not support mandating new reporting for nonprofit hospitals, which are required to submit annual cost reports and tax filings. The advocacy group has funded research that shows the savings from discounts go to patients. Hospitals enrolled in the program are much more likely to provide free care and specialty services, such as transportation, that are “typically not the ones you can use to pad your pockets,” she said.
Testoni said program growth is good because it means more care can be provided in outpatient settings and by safety-net providers for low-income populations. The bigger sales numbers, she said, could stem from more prescriptions or from higher drug prices. Detailed information about either metric is not public.
“Are we concerned that somehow pharmaceutical companies are being hurt by this?” Testoni said. “Because I’ve never seen any evidence of that in terms of their revenue going down or them having trouble keeping their doors open.”
‘Essentially Taking Over’
Hospitals aren’t required to prove that the large pharmacy networks serve uninsured or needy patients. The larger networks enrich the hospitals and the pharmacies, said Fein of Drug Channels.
A 2018 Government Accountability Office report found that a hospital or clinic generally pays a flat dispensing fee — typically from $6 to $15 — for each eligible prescription a pharmacy processed. And pharmacies can contract with multiple health care providers: One Walmart central fill facility in Spring, Texas, contracted with 1,842 340B hospitals and clinics, the InvestigateTV and KHN analysis found.
Recent securities filings for Walmart, Walgreens and CVS Health — the biggest players in the contract pharmacy market —- do not provide line-item detail on how many 340B prescriptions are processed or the revenue those transactions generate. Walmart did not respond to requests for comment. CVS declined to comment.
CVS reported in an August financial filing that operating income increased by a third between March and June compared with a year ago and noted that 340B business contributed to that increase but provided no further detail. The company acquired 340B contract pharmacy administrator Wellpartner in 2017.
Walgreens mentioned the program in its 2020 annual financial filing, noting that changes to government pricing and regulations “could also significantly reduce our profitability.” Walgreens spokesperson Rebekah Pajak said that many of the company’s stores are in underserved areas and that it is proud to help fulfill the program’s goals. She declined to disclose the dispensing fees or terms of its contracts with hospitals and clinics.
Karyn Schwartz, vice president of policy and research at PhRMA, called the 340B program a “black box” and said drug companies would like more transparency because they “really have no way of knowing” how hospitals and pharmacies use their discounts.

Drugmakers said they continue to participate in the program by sending direct discounts to the hospitals but have eliminated some or all of the discounts passed through contract pharmacies because they didn’t trust the transactions, according to emails the companies sent to KHN and InvestigateTV. Novartis, which announced last year that it would sell drugs at a discount only for pharmacies within 40 miles of a hospital, said there is a “complete absence of transparency” in the contracts between hospitals and pharmacies.
“Contract pharmacy arrangements benefit for-profit pharmacies, third-party administrators, other middlemen and hospitals,” Novartis spokesperson Caryn Marshall wrote in an email.
“Lilly welcomes reforms where patients are identified as 340B eligible at the point-of-sale and share in discounts under the program,” said Tarsis Lopez, Eli Lilly spokesperson.
Getting By on ‘Half a Dose’
Meanwhile, as businesses wage war over profits, patients are stuck. Andrew Kosowski, a 75-year-old retired police officer with diabetes, was shocked last year when he lost access to discounted drugs from 340B.
Kosowski is a patient at UnityPoint Health in Peoria, Illinois, which uses funds from the program to supplement the prescription costs of low-income and Medicare patients. Under 340B, many of his prescriptions were $15 each.
Without the discount, Kosowski’s insulin and other drugs had cost more each month than his Social Security check delivered. “I wasn’t going to spend that kind of money,” he said. He took “half a dose to get me by.”
He recalled how his feet hurt and his mind was affected without his full prescriptions.
PhRMA’s Schwartz declined to speak to Kosowski’s crisis but said the industry participates in 340B and would like to see direct patient benefit. “We hope policymakers step in and really clarify the role that for-profit pharmacies are supposed to be playing in this program and ensure that patients benefit,” Schwartz said.
Kosowski was fortunate to have an ally in Anne Webster, a nurse practitioner at UnityPoint who guided him through months of filling out forms to eventually qualify for financial assistance directly from Novo Nordisk.

The assistance, though, does not cover medications from other companies that he had gotten at the 340B discount price — medications that had helped him better manage his diabetes.
Webster said pharma’s standoff came at the worst possible time: “A Type 2 diabetic is so high-risk for mortality from coronavirus. And they require more insulin if they are ill with the virus.”
Kosowski is not her only patient missing prescriptions.
“I think I prescribed over 2,000 prescriptions in one year to the 340B program for my patients who are underinsured, not insured and are financially challenged,” Webster said.
KHN data editor Holly Hacker contributed to this report.
InvestigateTV is Gray Television’s national investigative team and provides innovative, original journalism from a dedicated investigative team and partners. InvestigateTV is available on AppleTV, Roku, Amazon Fire, at InvestigateTV.com and across Gray broadcast and digital media properties. Gray Television, headquartered in Atlanta, is the largest owner of top-rated local television stations and digital assets in the United States. Upon its anticipated acquisition of the television stations of Meredith Corp., Gray will become the nation’s second-largest television broadcaster, with television stations serving 113 markets that reach approximately 36% of U.S. television households.